

Leading with kindness
FEATURE – In this Argentinian hospital, leading with respect and kindness strengthened patient value, resilience, and culture, enabling sustainable growth and collective learning.
Words: Javier Sala
Our lean transformation story goes hand in hand with our leadership journey—after all, that’s where everything truly started and where it still lives today.
Instituto Modelo de Cardiología is a private, boutique healthcare institution in Córdoba, Argentina, that was established in 1977. We have 72 beds, more than 7,200 admissions per year, over 237,000 outpatient visits, and a 24/7 emergency department that alone sees more than 62,000 patients annually. We specialize in cardiology, but in reality, we are much more than that: 53 departments, ambulatory and inpatient care, high-complexity procedures, and patients referred from across the country.
One thing defines us: patients choose us. They are not assigned here. We have no captive insurance population. If we fail to deliver value—be it clinical, human, or operational—we simply stop existing. That reality shapes every leadership decision we made.
WHY LEAN BECAME A LEADERSHIP QUESTION
In 2012, our board asked a simple but uncomfortable question: “Why do we need Lean?” The answer wasn’t cost reduction, but survival with purpose.
Argentina’s healthcare context is volatile, with high medical inflation and fragmented reimbursement models (fee-for-service, bundles, pay-for-performance—all at once). Technology evolves faster than our ability to evaluate it responsibly. Treatments are increasingly expensive, and knowing when, for whom, and how to use them is a constant ethical and operational challenge.
At the same time, we were facing micro-level challenges: physician burnout, shortages in certain specialties, silo thinking, and people working simultaneously in multiple institutions with different cultures and values.
The board understood that if leadership did not change, nothing else would. Lean, for us, became a leadership system to protect patient value, support our people, and build resilience.
Our first decision was to start with leaders, rather than projects. We conducted leadership assessments and institutional evaluations with one core belief: if leaders were aligned to patient value, everything underneath could be improved. If they were not, no tool would save us.
We introduced model cells, beginning not with physicians, but with supporting areas—purchasing, scheduling, laboratories, pharmacy, billing, appointment centers. This was strategic. Physicians were skeptical, and we knew credibility would come from removing the daily frustrations that surrounded their clinical work.
Once those improvements became visible, physicians began to feel the difference and eventually engaged.
EDUCATION AS THE CORE COUNTERMEASURE
One of our biggest challenges was brutally simple: no one had been trained to think this way. Lean was not taught in medical schools, nursing programs, or technical education. Leadership training focused on expertise, not system thinking or change management.
So we invested heavily in education, as something that had to be part of leadership responsibility.
We ran leadership workshops. We did gemba walks with experts from the US, Brazil, Europe, and Japan. In 2016, we brought a cohort of our clinical leaders to the Academy for Excellence in Health Care at Ohio State. In 2018, we brought the Academy to Argentina so more leaders could learn together, on site.
Our message to leaders was consistent. We taught them to always start by asking what is best for the patient, to be curious (instead of defensive), to listen actively, to create psychological safety, to decide improvements based on impact and effort (not hierarchy), and to share results openly, internally and externally. More than anything, we encourage them to lead with kindness. Respect is not optional in healthcare.
BREAKING SILOS THROUGH SHARED LEARNING
Physicians are trained to excel individually, but Lean required us to learn collectively.
That’s why we built cross-functional teams where chiefs of cardiology, surgery, pulmonology, IT, HR, finance, nurses, pharmacists, and technicians learned together. We practiced A3 thinking, benefit–effort prioritization, and real gemba observation.
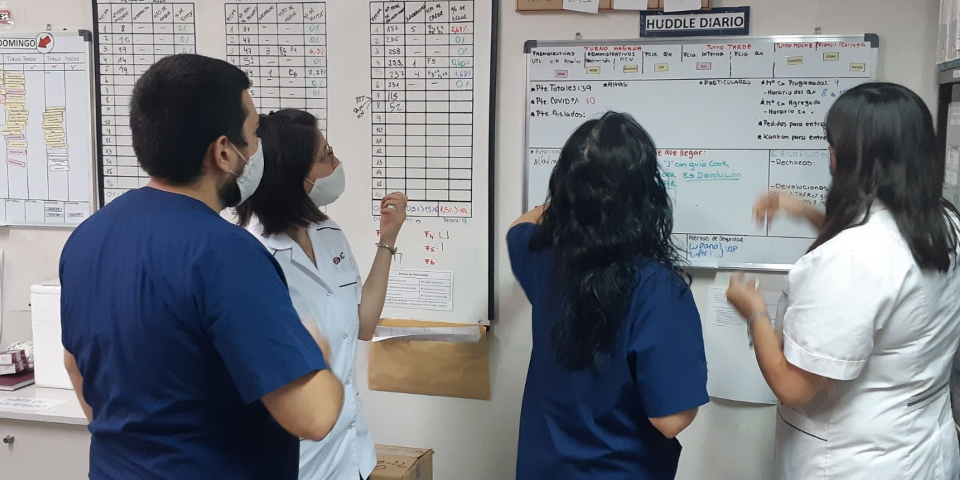
We emphasized yokoten—knowledge sharing. A pharmacy huddle became a learning space for lab teams. Central lab practices inspired outpatient flows. Knowledge started to move laterally, not top-down.
We also started learning directly from patients. Gemba walks following patient journeys—like ambulatory catheter procedures—revealed waiting, frustration, and waste that metrics alone could not show. We trained leaders to listen to four voices: the patient, the institution, the process, and the people.
OUR RESULTS
Over 12 years, we have seen great results. Without adding beds, we increased ambulatory visits by 66%, hospitalizations by 54%, and emergency visits by 92%. All while increasing staff by only 5%, and without compromising quality or safety. Patients continued to choose us.
But the deeper transformation was in leadership behavior. It’s been very gratifying to see leaders move from knowing to learning, from controlling to coaching, from imposing to co-creating, from results obsession to process discipline, from pushing change to building ownership, from evaluating to reflecting and learning. To me, that shift is the true measure of lean maturity.
As our confidence grew, we realized we had a responsibility beyond our walls. In 2018, we hosted the first Lean Healthcare Summit in Argentina and subsequently founded the Lean Institute Argentina inside the hospital. We also opened our gemba to others.
What mattered most to me personally was seeing board members sit through an entire lean summit, as learners. That visible commitment is what made all this possible.
Lean is a choice leaders make. Hospitals must adopt Lean to add value to patients, professionals, payers, and the health system. But that only happens when leaders design systems that nurture respect and curiosity, build organizations that learn faster than the world changes, and preserve core values while adapting relentlessly.
For us, those values are simple and non-negotiable: the patient always comes first.
THE AUTHOR

Read more


FEATURE – Lean healthcare is new to China. The authors share some examples of improvements projects taking place in Chinese hospitals, which they hope will inspire more organizations to take lean on.
NOTES FROM THE GEMBA – In the last article about Aramisauto’s transformation, the author discovers how Lean shapes the website behind millions of customer interactions every month.

OPINION – A new publicly owned open-source technology promises to make direct, unmediated trade relations trustworthy, opening the door to an era of democratization and cooperation in global commerce.

CASE STUDY – Thousands of kaizens, a relentless focus on learning and the determination to continuously improve have made of this Norwegian company something of a lean fairytale.
Read more
CASE STUDY – This hospital in Argentina has leveraged the power of Lean Thinking to greatly enhance patient care, even in the pandemic, and receive internationally renowned accreditations.

ROUNDUP – Our editor reflects on the all-important lean concept of “respect for people” and shares some of the best content published by Planet Lean on the subject.
FEATURE – Using Carol Dweck’s distinction between fixed and growth mindsets, the author discusses how leaders should think and act to make lean possible. Looks like no fixed mindset is beyond saving.

INTERVIEW – PL sits down with a consultant and a manager from the St Elisabeth hospital in the Netherlands to talk about the organization’s “loving care” approach to treating patients.