

Fighting Covid-19 with lean healthcare
FEATURE - A Lean Global Network team of lean practitioners and coaches shares a set of lean healthcare tips hospitals can use today to support their battle against Covid-19.
Words: Cristina Adalid Fontcuberta, Flávio Battaglia, Denise Bennett, Oriol Cuatrecasas, Alice Lee, Dr Carlos Frederico Pinto and Dr Javier Sala Mercado.
The Covid-19 pandemic is pushing healthcare systems around the world to the limit and, despite the heroic effort of healthcare professionals, hard work is often not enough. The images coming from the most heavily affected areas tell us of Emergency Departments filled to the brim, hospitals struggling to treat everyone due to the very high number of people that the virus sends to the ICU, and exhausted staff who are often forced to work without adequate protective gear.
As the Global Lean Healthcare Initiative, we are supporting healthcare organizations around the world as they apply lean thinking and practice in coping with this crisis. Sharing our thinking across four continents, we have come up with seven key lean practices - each with a set of actionable tips - that can really help a healthcare team handle this emergency more effectively.
- Design the patient flow
- Visual Management
- Standard work to ensure safety, quality and efficiency
- Engage in short, structured communication cycles
- Build skills fast with a people-development plan
- Review priorities to ensure capacity
- Level capacity and protect staff
1. Design the patient flow
- Understand demand and pace for each patient flow.
- Visually map your newly-designed flows and processes to better understand and share.
- Physically segregate flows and ensure that critical patients have access to dedicated resources, so that they don’t cross paths with other patients. Separate those with respiratory symptoms from those without. Minimizing the number of flow groups reduces complexity as we move patients through the system.
- Develop a plan for every flow: for example, Covid patients with mild symptoms and Covid patients with severe symptoms.
- Encourage “pull”, by having downstream care providers actively look for their next patients in order to move them to the right place as fast as possible. Pulling patients from ICU into an available bed will allow the next patient to flow in. If possible, maintain some downstream capacity for outflow.
- Assign highly skilled professionals to the intersections of the flow and to areas making key decisions (like Triage).
EXAMPLE 1 - ARGENTINA In a hospital in Cordoba, to separate the flow of Coronavirus patients from that of regular patients, we have converted the cardiac rehabilitation center into a dedicated Covid-19 space. In this area (located in a separate building), we have mapped the flow of patients, physicians, nurses, technicians, materials and information and made several improvements, in order to reduce exposure and reduce the number of PPE per patient seen. We know that when the number of infections ramps up and severe or critical cases arrive, we will have to bring Covid-19 patients into the hospital. That’s when we will separate and isolate entire areas in three different stages to avoid any risk of further spreading the infection.

EXAMPLE 2 - SPAIN This simple graphic maps the process that is followed for Covid-19 patients in a hospital in Catalunya.

EXAMPLE 3 - USA A community health center in Massachusetts has reorganized its work streams across different locations to reduce infection risk for staff and patients.

2. Visual management
- Share clear and visual work instructions for the critical steps in the process, so that everyone knows what to do and how.
- Place visuals at each bed to minimize the time to obtain the necessary information. The goal is to create visuals that provide needed information in seconds, at-a-glance.
- Use different color codes for areas, pathways, classifications to make clear the current standards, like the purpose of an area, can change quickly and pathways can be extended or reduced overnight. This way, everybody is kept up to speed with the evolving situation.
- Train professionals quickly using simple visuals.
- Incorporate visual management in your communication.
EXAMPLE 1 - AUSTRALIA The team in the Australian hospital has filled its “command centre” and surrounding corridors with whiteboards to increase transparency of planning. Now one can immediately see what is going on and what the team is up to, which helped with connection and dependencies. They combine this with regular huddles where they review key metrics, progress against visual master Gantt chart, critical work-in-progress and they address barriers. They visualize the work for today and allocate help. The staff’s FAQs are visualized, too, along with a status of supplies. All patient flows for COVID-19 are mapped and visual. They make changes in real time on the maps as they continue to develop their thinking on how these patients should be flowed and cared for. Other teams regularly go to see what they are working on, to test out thinking and contribute. Connecting silos of front-line and leadership planning has been made both more effective and efficient by making things visible.
EXAMPLE 2 - ARGENTINA In an Argentinian hospital, visual, easy-to-understand instructions on how to don PPE during Covid-19 testing are posted on the walls but also inside the testing kits (on the inside of the lid) - to ensure biochemists don’t miss any steps.

EXAMPLE 3 - SPAIN Checklist on each bed, to ensure professionals have all the information they need available at the place of work.

3. Standard work to ensure safety, quality and efficiency
- Develop standardized work and train teams in using those standards, to guarantee safety and agility in your operations.
- Observe the work and assess adherence to standards.
- Organize people (both management teams and care teams) in small integrated teams - doctor, nurse, assistant doctor, etc - instead of big groups of professionals, to share vital information more quickly.
- Limit the movement of staff by organizing your space into dedicated areas for the different teams.
- Enable leaders to identify priorities and necessary actions using Leader Standard Work. In a crisis, it is a good idea to create a central hub (incident command center) for information flow with visual management of key work streams (e.g. resource management of PPE; staff status – exposed and quarantined, tested positive, replacement requests; etc). Leaders focus the teams with structured and frequent huddles.
EXAMPLE 1 - AUSTRALIA Executive leaders in the Australian hospital attend each site huddle daily to show respect and communicate directly with staff.
EXAMPLE 2 - SPAIN These colored tags, in use in a Barcelona hospital, indicate different areas healthcare professionals are deployed in. When a doctor/nurse tests positive to Covid-19 and has to go home for self-isolation, they place their tag into this plastic folder. This tells the team immediately who needs to be replaced. (As of April 6th, around 19,400 healthcare workers have been infected with the Coronavirus in Spain.)

EXAMPLE 3 - USA A healthcare organization in Massachusetts has organized their senior leaders and managers into two parallel teams that are dedicated to two separate areas of the organization to reduce the possibility of cross infection throughout the larger management team and to preserve human capacity. This model was soon replicated with segmented care teams.
EXAMPLE 4 - ARGENTINA The Cordoba hospital’s Crisis Committee developed a set of Covid-19 guidelines that can be accessed at any time via an URL code posted throughout the organization or a link the healthcare workers have installed on the cell phones. These guidelines include definitions, protocols, flow charts, standard processes, etc. Most importantly, they represent a “dynamic” document that is constantly updated as new evidence/information becomes available and as the team is called to face up to new challenges (particularly important in this situation, because this a new disease that we need to learn about fast).
EXAMPLE 5 - BRAZIL In a hospital near Sao Paulo, all the material necessary to intubate Covid-19 patients is organized in a ready-to-use standard kit.

4. Engage in short, structured communication cycles
- Implement a daily management system to structure periodical meetings, short in duration, at all management levels as a way to prepare people for the specific situation of a shift or day. Hold these huddles in each work stream. The huddles may be virtual if teams are segregated.
- Create visual boards to act proactively and preventively by visually anticipating important decisions in the face of difficulties, which will change every day.
- Encourage people to communicate problems, difficulties and opportunities for improvement at all times.
- Enable better communication by always working in teams.
EXAMPLE 1 - AUSTRALIA The Daily Management System in use in this hospital has been critical to ensure that front-line teams engage daily in conversations about their concerns. We have increased the focus on front-line huddles to create more structure and collect concerns, feedback and critical information every day. The ward huddle is now split into two: safety huddles at the start of the shift (duration of 5 minutes) and top-tier leaders’ huddles to close the loop of information and respond to team members’ concerns. This creates a time for the teams to reset and connect during these stressful work days. Huddles have proven such an important part of communication and supporting each other. The team had to redesign huddles to keep staff safe and adhere to the social distancing requirements using a combination of technology and visual marks on the floor to help us maintain the social aspects of the huddle process.

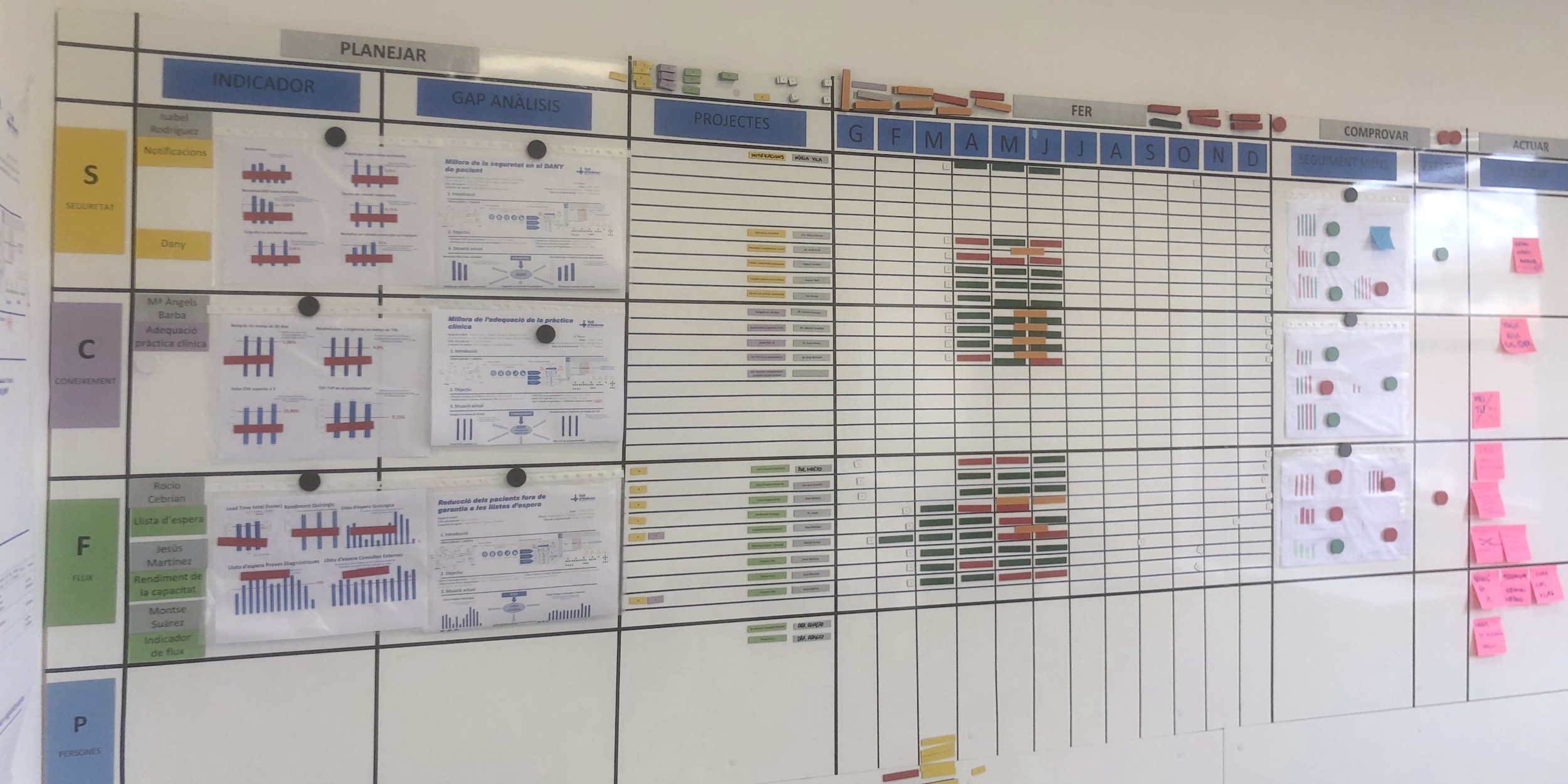
EXAMPLE 2 - SPAIN The panel in use at the “command center” in a Catalan hospital, with different colors referring to different areas tackling the Covid-19 emergency. The board is updated daily/weekly as the situation evolves.

EXAMPLE 3 - SPAIN These symbols are used to visually identify Covid-19 positive patients and those awaiting test results. The star sign indicates the patient’s family has been informed.

5. Build skills fast with a people-development plan
- Plan for how you onboard and train new team members. As doctors who left for non-hospital work or retired doctors come back into hospital service, together with other specialty physicians or new medical school graduates, you will need to provide orientation and knowledge to enable them to be productive as quickly as possible.
- Leverage visual standards to train quickly and run on-the-spot assessments to evaluate attainment of the standard.
- Bring the right knowledge to professionals - no more, no less. Not everyone needs to know everything at once, to avoid information overload and make it clear what people should focus on. At the same time, transparency is key and everyone should be giving the lowdown on what’s happening in the organization.
- Take the time to capture lessons learned each day in a structured way (i.e. through the huddles). It can save you a huge amount of time tomorrow as you further improve and learn. Learning is one of the most precious things that happens in burning platform situations.
- Recognize the importance of every small improvement and understand that quick action accompanied by quick course correction (as you learn what works best, through rapid-cycle PDCA) is the way to achieve success.
EXAMPLE 1 - ARGENTINA Chinese research on the virus indicated fever and cough as the main symptoms of the infection, but there have been several covid-19 cases in the USA and Argentina that showed different symptoms (such as headache, fatigue, diarrhea and less cough). The virus might express itself in different ways in different places, which is why it’s important to capture data. In a hospital in Argentina, for each suspected Covid-19 patient (we have a 24-hour delay to the PCR results), the team is using tablets to record symptoms in each examination room and then uploads them on a simple document on Google Drive. This information (what symptoms, how long they took to appear, etc) is updated in real time and we expect it to be incredibly useful for us to learn quickly.
EXAMPLE 2 - SPAIN Visuals to train the different teams on each of the stages and main operations for ventilation, and when to do it.

6. Review priorities to ensure capacity
- Cancel and reschedule all non-urgent appointment and elective procedures. If appropriate, some of these patients can be seen using telehealth.
- Keep most patients away from the ERs and do triage and testing outside/elsewhere.
- Redirect teams from other areas of the hospital to bring support to the most critical flows.
- Place younger professionals on the front-line interaction with patients and older and at risk ones in the back office and assigned to telehealth support of patients.
- Estimate the expected number of non-Covid emergencies using historical data.

EXAMPLE 1 - USA In Massachusetts, a 160-bed community hospital has been converted into a dedicated Covid-19 hospital - the first one in the USA to segment the patient population further and prevent further spread in the patient and staff community within a hospital. This also keeps the city’s EDs and hospitals operational with needed capacity for other acutely sick patients with lower risk of infection. They do triage and testing in a mobile tent outside in their parking lot. Other countries, like South Korea and the UK, have created drive-through testing centers.
EXAMPLE 2 - USA A hospital in Massachusetts has partnered with an outpatient community health center to care for their non-Covid patients to keep the patient flows clear and distinct.
EXAMPLE 3 - ARGENTINA A hospital in Cordoba - providing care mainly to cardiovascular patients (more than half of the total number), a category at high risk complications from a Covid-19 infection - has analyzed its 2019 monthly/seasonal demand in the ER to understand what they can expect in terms of emergencies (strokes, infarctions, etc) over the coming weeks. This is helping them to prepare for the Covid-19 emergency.
7. Level capacity and protect staff
- Give people the time to recover. This is important to avoid staff burnout and the mistakes that often result from it. Limit working hours, creating a smarter shifts plan so that the teams are able to “run the marathon”.
- Assign tasks by balancing staff (which should include age, empathy, energy, mental strength, knowledge…) and try to cross-train staff in more than one area of the organization as these multi-skilled workers can be moved where they are needed for flexibility.
- Create a plan for managing different levels of capacity (for example, as you add new ICU beds to your Covid-19 flow). As your demand increases, gradually devise new plans on how machines/equipment/spaces are going to be used/moved/assigned each time. Allocating all resources from the beginning could result in not using them effectively; it could also make each potential mistake much more damaging. Conversely, a plan with several iterations allows you to integrate your lessons learned and improve your response.
- Calculate how much material you need for each flow, process, scenario.
- Don’t be afraid to start from scratch - set up the space using workplace organization techniques like 5S and 3P and create standards for each flow/process/scenario.
- Ensure material is always available to professionals when they need it. It is key to reduce searching for things as, in hospitals, hours are typically spent walking and searching for materials. Always have someone responsible for replenishment and make sure you are making the most of the material you have.
EXAMPLE 1 - ARGENTINA For the first time since 1977, physicians in the Cordoba hospital are working no longer than 12 hours and nurses no longer than 8 hours. As of March 28th, front-line staff - younger than 60 years old - has been divided into three groups: the first two groups work for five days (one from 8 AM to 8 PM, and the second from 8 PM to 8 AM); after that, the night shift goes home and stays in quarantine for five days (in case any Covid-19 symptoms appear) and the third group comes in. The day group will move to the night group, and so on. Additionally, we have a plan for managing different levels of Covid-19 patient demand and have decided how the different areas (i.e. ICU) will be converted for Covid-19 care in three stages.
EXAMPLE 2 - USA A ICU nurse in Boston noted how many PPEs she and her fellow nurses had to use as they entered and exited ICU rooms to adjust or respond to IV pumps. She proposed, got approved and tested the process of moving all the IV pumps outside the rooms, at the door, to preserve PPE use and make it faster for nurses to do this part of their work. Obviously, the nurse would still don PPE and check on their patients and IV site, but this way they can reduce the number of times they need to enter/exit rooms (like when pumps beep).
EXAMPLE 3 - BRAZIL A hospital in our network has come up with a three-tiered plan to prepare for the different stages of the Covid-19 crisis.

EXAMPLE 4 - ARGENTINA After their first suspected Covid-19 case - hospitalized on March 23rd - turned out to be negative, the hospital in Cordoba realized a large number of PPE had been used (unnecessarily) to isolate the patient from caregivers and decided to review its process to minimize staff exposure and PPE utilization. They mapped all the touch points for that first patient over the 24 hours he awaited results and merged or eliminated some - going from 23 touch points per patient every 24 hours to 7-9 touch points with two patients in inpatient rooms. For their first confirmed Covid-19 case, hospitalized on March 29th, the team had 10 touch points with a 57% reduction in PPE usage over 24 hours, for three consecutive days. For ICU patients, the original design started a 60 touch points per patient every 24 hours and is now the expected to be around 20 touch points every 24hs for seven Covid-19 ICU patients.This was achieved by deploying highly skilled professionals to the relevant areas and by implementing a Kanban replenishment system.

LEAN VS. COVID-19
The transformations we facilitate typically take years to complete, but they are accomplished by taking immediate action, day after day, as the circumstances around us change. Indeed, Lean Thinking can lead to great results very quickly - which is exactly what healthcare organizations around the world need right now.
We hope this article will reach healthcare professionals around the globe, especially those who have never even heard about Lean Thinking, as they prepare for an onslaught of Covid-19 cases. To lean neophytes, we say: some of these suggestions might be very different from your regular way of working, but we ask you to give them a try. They might even take a little bit of time to implement (we know how precious a resource time is right now), but we urge you to see this as an investment in your ability to face the upcoming challenges posed by Covid-19. We have decades of combined experience transforming healthcare organizations and believe that these measures can make a big contribution in the fight against this threat.
Our collective goal is currently to “flatten the curve” - slowing down the spread of Covid-19 so that we can level the caseload for hospitals, allow them to save more lives and have the time to get them the extra supplies and equipment they need. In lean terms, this is clearly a global heijunka problem with far-reaching consequences on our healthcare systems. The PPE debacle unfolding in many of our countries suggests this crisis will also force us to rethink the way we produce and handle the logistics of key equipment. We believe that Lean Thinking has a lot to contribute to this debate, as the world tackles this emergency and then starts to reimagine life after the pandemic.
For more lean healthcare inspiration, click here.
This article is also available in Spanish, Portuguese, Italian, Dutch, Polish, Hungarian, Chinese and Russian.
THE AUTHORS

From the top left: Cristina Adalid Fontcuberta, Instituto Lean Management, Barcelona; Flávio Battaglia, Lean Institute Brasil; Denise Bennett, Lean Enterprise Australia; Oriol Cuatrecasas, Instituto Lean Management, Barcelona; Alice Lee, Lean Enterprise Institute, Boston; Dr Carlos Frederico Pinto, Instituto de Oncologia do Vale, Brazil; Dr Javier Sala Mercado, Instituto Modelo de Cardiología Privado, Cordoba, Argentina.
Read more

CASE STUDY – Catalonia’s largest hospital is undergoing a successful transformation – supported by pioneering hoshin experiments – that has already turned it into a poster child for lean healthcare in the region.

INTERVIEW – This cardiac laboratory in Singapore was targeting one improvement and ended up with something different, but equally impactful for its patient flow.

CONTENT ROUNDUP - Happy New Year, readers! Before kicking things off for 2017 with new, original content, we wanted to share with you the Top 10 of the most-read Planet Lean articles from last year.

FEATURE – Variety in sensei approaches can cause a lot of confusion. The author sheds light on the subject by describing a sensei’s five modes of interacting with individuals and teams.